For those who have experienced prolonged childhood trauma, the concept of dissociation, or distancing yourself from your memories, emotions, and experiences, may feel very familiar.
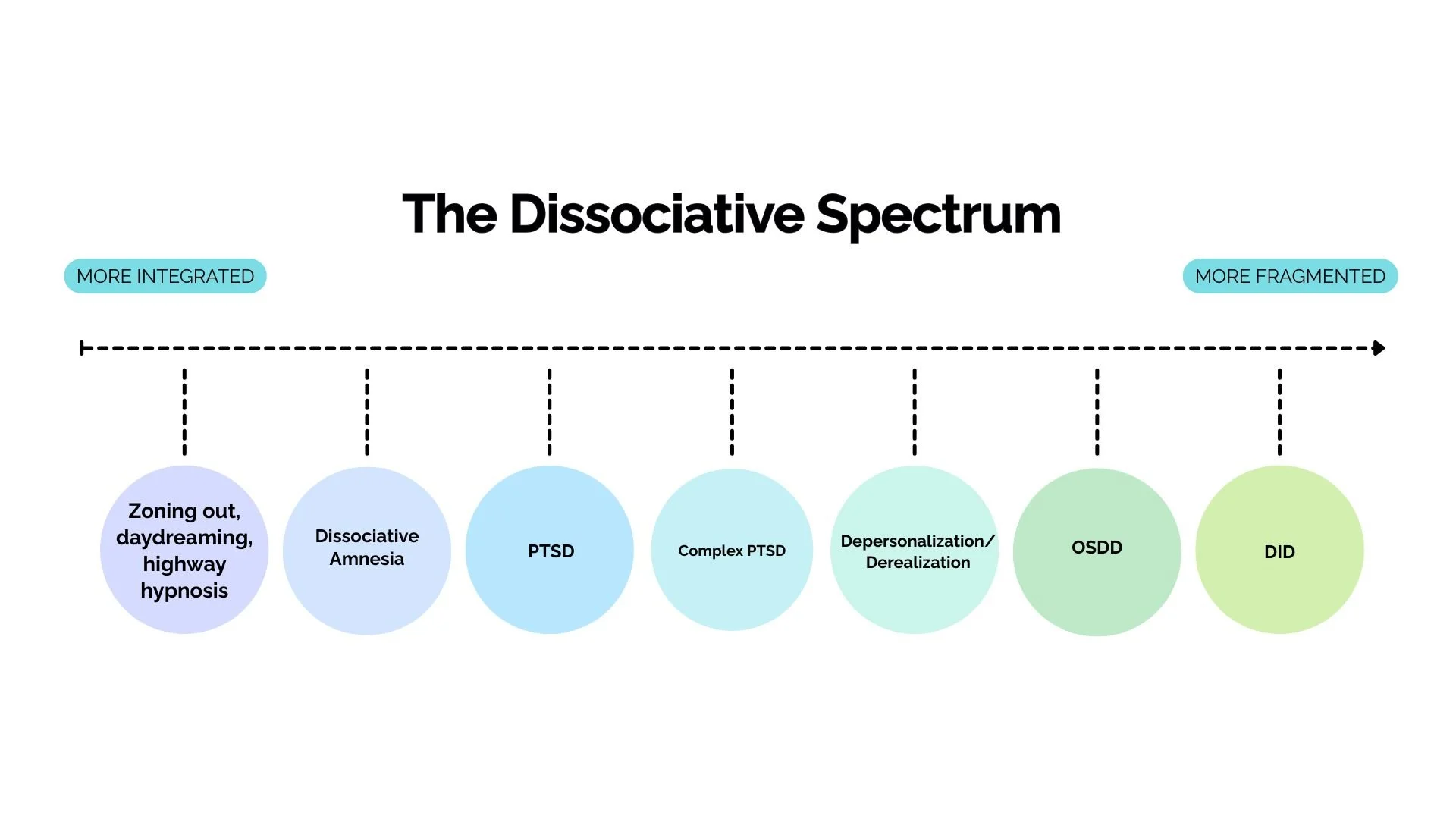
Dissociation exists on a spectrum, ranging from “normal” daydreaming to diagnosable conditions such as Depersonalization/Derealization (DPDR), Other Specified Dissociative Disorder (OSDD), and Dissociative Identity Disorder (DID).
Maybe you have experienced:
Gaps in your memory
Feeling as though you are fragmented
Internal voices or loud thoughts
Intrusive thoughts or urges
Intense flashbacks
Disconnection from yourself, other people, or the world around you
Challenges with relationships, work, or overall functioning
Dissociation and Dissociative Disorders
Regardless of where you are on the spectrum, you may be finding that the dissociation that was so vital to your survival is holding you back in other ways. You may want deeper connections with others, more even emotions, and a better relationship to your past.

Treatment
If you have had a bad experience with therapy in the past, it may be because your therapist was not fully taking into account your dissociation. I know because I’ve been that therapist before! Therapy for dissociation includes the following elements:
Getting to know your parts, building trust with them, reducing any conflict between them, and getting their permission before moving forward with trauma reprocessing
Intentional and gradual trauma reprocessing, often beginning with more peripheral, recent, or “easier” elements as opposed to an entire traumatic memory
Continued attention to symptom stabilization, grounding, and pacing
Integration of therapeutic work outside of session, allowing you to build a life worth living
Seeking therapy for dissociation can be scary, especially if you haven’t had a great experience before. If you’re ready to learn more or have questions, don’t hesitate to reach out below.
Frequently Asked Questions
-
If you’ve noticed symptoms aligned with dissociation, many start by completing the Dissociative Experiences Scale, or DES. This is an initial screening tool and cannot be used to diagnose, but it can highlight symptoms that can be further assessed.
The two assessment tools used to diagnose dissociative disorders are the Multidimensional Inventory of Dissociation (MID) and the Structured Clinical Interview for Dissociative Symptoms and Disorders (SCID-D). These assessments are more thorough than the DES, and together with your therapist’s assessment can provide more specific diagnostic clarity.
-
No! Some parts may fuse as the result of trauma work, but it is not necessary for healing. The primary goal of “integration” is a higher degree of cooperation between parts, not the disappearance of parts altogether.
-
Yes! In the case of memory gaps and dissociation, we often begin with the present-day, downstream effects of trauma, rather than the trauma itself. As such, having explicit, narrative memory of traumatic events is not required for therapy to be effective.
-
Maybe! Some people find that as we build trust with protector parts and progress through trauma therapy, more memories come back to them. However, memory is an incredibly complex thing, and it would be impossible to guarantee that certain memories will come back to you, or that they will be accurate if they do.
-
EMDR must be significantly adapted for working with complex trauma and dissociative disorders. I utilize the Progressive Method and weave in parts work for this. Here are a few high-level differences:
We work far more extensively to establish stabilization before reprocessing any past memories, especially in getting to know your parts
We begin reprocessing more recent or peripheral events, and we ensure that all parts of you are on board with the work we are doing
We often use shorter “sets,” meaning that the exposure to the distressing material is much shorter compared to standard EMDR